
For more than 3000 years, alcoholic beverages have been consumed in multiple societies through the centuries and cultures. Pulverized antimony was used as eye shadow by Egyptian women and named al-Kol. In the 16th century Paracelsus Theophrastus Bombastus from Hohenheim used this term for distilled liquor and called it alcohol [15].
- The final process of ACM is the result of dosage and individual predisposition.
- That also may involve supportive care that will help prevent — or at least reduce the impact of — any alcohol withdrawal symptoms.
- Echocardiogram usually reveals left ventricular hypertrophy, depressed left ventricular ejection fraction, and dilation.
- It showed a significant increase in both acute and chronic alcohol intoxication.
- Your doctor will also ask you about your medical history and drinking habits.
3. Ethanol-induced Heart Fibrosis

Although these reports were isolated, the routine use of propranolol and subsequently all β-blockers were considered relatively contraindicated in treating cocaine-induced cardiovascular emergencies. As a result, benzodiazepines have been the drug of choice in treating the cerebrovascular and subsequent systemic hyperadrenergic complications of cocaine, and nitroprusside or phentolamine being advocated for peripheral vasodilatory effects. It is now becoming apparent that treatment of cardiovascular effects of cocaine should involve a multifactorial approach to combat both central nervous system and peripheral vasospastic effects of cocaine. The risk of developing alcoholic cardiomyopathy appears to be related to both the amount and duration alcohol intake.
Clinical work-up for alcoholic cardiomyopathy

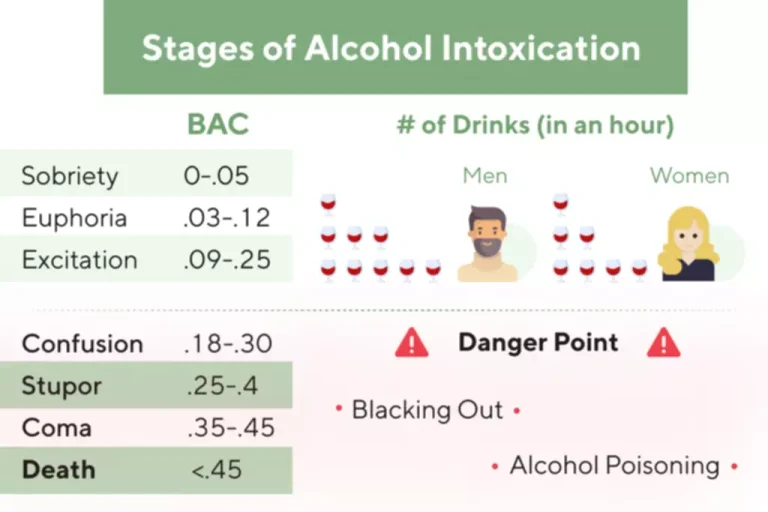
The guidelines typically define one drink as specific quantities for different types of alcoholic beverages. For instance, a single drink of beer is typically considered as a 12-ounce (355 ml) serving of regular beer, usually containing around 5% alcohol by volume (ABV). When it comes to wine, one drink is defined as a 5-ounce (148 ml) serving, which typically contains about 12% ABV. Distilled spirits, such as vodka, whiskey, rum, or tequila, are measured as 1.5 ounces (44 ml) per drink, with a typical ABV of around 40%. It is important to note that the size and strength of different alcoholic beverages can vary, so these definitions serve as general guidelines. It is always advisable to be mindful of individual tolerance and consume alcohol responsibly [4-6].
Is there an immediate risk of alcohol intake?
- Furthermore, alcohol consumption has also been classified in the literature by ranges of consumption as mild, moderate, and heavy drinking.11 In this regard, these categories have the following consumption thresholds that also differ according to sex.
- They also have not established how long a person would need to consume alcohol before developing ACM.
- More specifically, atrial fibrillation with rapid ventricular response is a cause of arrhythmia-induced cardiomyopathy,61 which can potentially worsen LVEF in AC patients, on top of the direct toxic effect of ethanol, acetaldehyde damage, or the aforementioned genetic factors.
- In addition, contractile sarcomere proteins such as Myosin, Actin, and Troponin are also affected by ethanol, causing the functional progressive depression of myocyte contractility, inducing progression to heart failure [56,104,131].
Until the second part of the 20th century, there was no scientific evidence on the direct and dose-dependent effect of ethanol on the heart as cause of ACM [6,38]. However, there is a clear personal susceptibility of this effect that creates a wide variability range and alcoholic cardiomyopathy supposes significant inter-individual differences [50,66]. In fact, ACM is considered to be the result of dosage and individual predisposition [32]. It has been said that ethanol is the “perfect drug” because of its pleasant effects but damaging long-term effect [1,6].

Occidental Berberi is the term used for the clinical scenario caused by thiamine deficit, a situation commonly present in chronic alcohol misuse, and was attributed as the cause of ACM [68,69]. Similarly, electrolyte (Na, K, Ca, Mg, P) deficiencies or disturbances may play a major role https://ecosoberhouse.com/ in cardiac function, and ethanol misuse may be related to them [52]. Selenium deficit (Keshan disease in China) could also induce ACM in specific areas [70]. Based on epidemiological evidence, ACM is recognized as a significant contributor to non-ischemic DCM in Western countries.

What can I expect if I have this condition?
ACM produces a progressive reduction in myocardial contractility and heart chamber dilatation, leading to heart failure episodes and arrhythmias. Pathologically, ethanol induces myocytolysis, apoptosis, and necrosis of myocytes, with repair mechanisms causing hypertrophy and interstitial fibrosis. Myocyte ethanol targets include changes in membrane composition, receptors, ion channels, intracellular [Ca2+] transients, and structural proteins, and disrupt sarcomere contractility. Cardiac remodeling tries to compensate for this damage, establishing a balance between aggression and defense mechanisms. The final process of ACM is the result of dosage and individual predisposition.
- The clinical features of ACM develop when the injury is irreversible and advanced.
- For a comprehensive overview see Table 2 with combined data from [6, 8, 24, 28].
- Of the 56 patients included in the study, 28 were former drinkers and 28 continued consuming alcohol during the study.
- If you have the condition, your healthcare professional might recommend that your family members be checked.
- These chambers are important as they do the majority of the work of your heart, with the right ventricle pumping blood to your lungs and the left ventricle pumping blood to your entire body.
- Alcohol abuse has a toxic effect on many of your organs, including the heart.
- They try to control myocardial remodeling to avoid the progression of myocyte hypertrophy [39,148] or fibrosis [149] and ventricle dysfunction and dilatation, as well as to increase the degree of myocyte regeneration [150].
- Although some studies have detailed structural and functional damage in proportion to the amount of alcohol consumed during a patient’s lifetime[24], a large majority of authors have discarded this theory[21-23,25].
- Although physicians are aware of this disease, several pitfalls in the diagnosis, natural history, prognosis and treatment are still present.
- As the clinical use of propranolol increased, reports of accentuation of cocaine-induced hypertension and myocardial ischemia began to surface, blaming the unopposed alpha effects of the β-blockers.